Lincolnville tick bite lands Rockport man in hospital
") Steve Hand, of Rockport, remains in recovery from an April 20 tick bite that put him in the hospital for five days. (Photo by Lynda Clancy)
Steve Hand, of Rockport, remains in recovery from an April 20 tick bite that put him in the hospital for five days. (Photo by Lynda Clancy)
 “The term tick bite may be misleading as ticks do not bite and depart or feed rapidly like a mosquito. Ticks attach and feed gradually over a period of several to many days. Once a tick
has found a suitable place to feed, it grasps the skin, tilts the body at a 45-60° angle, and begins to cut into the skin with the paired chelicerae.” — Source: Tick Management Handbook An integrated guide for homeowners, pest control operators, and public health officials for the prevention of tick-associated disease
“The term tick bite may be misleading as ticks do not bite and depart or feed rapidly like a mosquito. Ticks attach and feed gradually over a period of several to many days. Once a tick
has found a suitable place to feed, it grasps the skin, tilts the body at a 45-60° angle, and begins to cut into the skin with the paired chelicerae.” — Source: Tick Management Handbook An integrated guide for homeowners, pest control operators, and public health officials for the prevention of tick-associated disease
 Source: Tick Management Handbook An integrated guide for homeowners, pest control operators, and public health officials for the prevention of tick-associated disease
Steve Hand, of Rockport, remains in recovery from an April 20 tick bite that put him in the hospital for five days. (Photo by Lynda Clancy)
“The term tick bite may be misleading as ticks do not bite and depart or feed rapidly like a mosquito. Ticks attach and feed gradually over a period of several to many days. Once a tick
has found a suitable place to feed, it grasps the skin, tilts the body at a 45-60° angle, and begins to cut into the skin with the paired chelicerae.” — Source: Tick Management Handbook An integrated guide for homeowners, pest control operators, and public health officials for the prevention of tick-associated disease
Source: Tick Management Handbook An integrated guide for homeowners, pest control operators, and public health officials for the prevention of tick-associated disease
Source: Tick Management Handbook An integrated guide for homeowners, pest control operators, and public health officials for the prevention of tick-associated disease
Steve Hand, of Rockport, remains in recovery from an April 20 tick bite that put him in the hospital for five days. (Photo by Lynda Clancy)
“The term tick bite may be misleading as ticks do not bite and depart or feed rapidly like a mosquito. Ticks attach and feed gradually over a period of several to many days. Once a tick
has found a suitable place to feed, it grasps the skin, tilts the body at a 45-60° angle, and begins to cut into the skin with the paired chelicerae.” — Source: Tick Management Handbook An integrated guide for homeowners, pest control operators, and public health officials for the prevention of tick-associated disease
Source: Tick Management Handbook An integrated guide for homeowners, pest control operators, and public health officials for the prevention of tick-associated disease
ROCKPORT — Steve Hand is not a man who gets tired, but last month he was wiped out. He made a visit to the third floor of the Knox Mill in Camden in mid-May, and when it came time to leave, he walked slowly to the elevator, shaking his head — “I won’t make it down the stairs.”
Normally robust, this is a man always on the move: He flies regularly from one end of the country for work, staying up late in airports and returning back to Rockport early in the morning to play or coach hockey, go turkey hunting, fish or dance in the evening with his wife, Amy. He is not one to get floored by a bug, let alone a little tick.
But he did, and it was bad enough that he spent five days at Pen Bay Medical Center getting pumped with fluids and antibiotics. After several weeks of symptoms, and trips in and out of doctors’ offices, the cause of his misery was finally diagnosed as anaplasmosis, an illness caused by the bacteria anaplasma that lives in the bellies of ticks.
Almost eight weeks later, Hand is still recovering. He is now 70 to 80 percent back to his normal state of health, but for a while, it was a hard row, with even his mind in recovery. Usually, he is quick on the draw, and can explain concepts and ideas with analogies that spark to his tongue. But for weeks following his bout of illness, his brain drew a blank.
“I was losing my train of thought, which I don’t normally do,” he said.
From bite to disease
On April 20, Hand was working at his rental property in Lincolnville when a small tick crawled up his leg, attaching itself to his thigh. It was a deer tick, he concluded.
Questions about ticks, bites, symptoms?
Don’t hesitate to call the Maine Department of Health, says Megan Kelley, Maine CDC epidemiologist. She encourages phone calls and emails. She wants the public to be educated.
Call 800-821-5821
“Ticks are generally found in brushy or wooded areas, near the ground; they cannot jump or fly,” says the Maine Center for Disease Control, in its guide, Tick-borne Diseases in Maine, a Physician’s Reference Manual. “Ticks are attracted to a variety of host factors including body heat and carbon dioxide. They will transfer to a potential host when one brushes directly against them and then seek a site for attachment.”
The website What Eats is a little more illustrative: “The tick attacks its host by waiting patiently on bushes or other vegetation with its front legs waving in the air until an animal or person passes by and brushes against it. Then, the tick hooks onto the other creature’s fur or skin with its legs and begins crawling around in search of a tasty place to bite.”
The eight-legged parasite is a relative newcomer to Maine, moving up the coast from southern New England over the past 20 years and increasingly prevalent, especially along the Midcoast. And ticks are wreaking havoc along the way, whether it is a deer tick, dog tick, or lone star tick. They carry pathogens that harm animals and humans — bacteria, viruses and protozoa.
Dog ticks in Maine are not currently thought to cause human diseases in the Midcoast because there is no Rocky Mountain Spotted Fever in Maine. Though, specialists hedge their bets, saying that, too, could change.
“Between the dogs and us, we’re pulling them off, 20 ticks a year, I bet,” said Hand. “You know the Bog in Rockland? I hear there is a spot where you walk 10 feet and you get 10 ticks on you.”
It is thought that the increase in ticks results from the growth of woods over the last century, which followed extensive clear-cutting during the 1800s. When habitat — trees and vegetation — were cleared for farms, so too the tick hosts, primarily white-tailed deer, lost their habitat. But with the regrowth the number of deer, and ticks, has increased.
According to the Tick Management Handbook An integrated guide for homeowners, pest control operators, and public health officials for the prevention of tick-associated disease (see attached PDF or click on the link), “ticks that may have survived on islands off the southern New England coast were able to increase and spread.”
The handbook, written by Kirby C. Stafford III, Connecticut’s Chief Entomologist at the Connecticut Agricultural Experiment Station, in New Haven, delivers much straightforward information in 80 illustrated pages.
Diseases acquired from tick bites have increased over the past decade, not only with the number of cases, but the types of tick-borne illnesses themselves.
Lyme disease is now but one of many tick-borne infections that lab workers scrutinize human blood samples for across the country. In Maine’s Midcoast, the incidence of anaplasmosis alone has tripled over the past three years.
In 2012, Knox and Lincoln counties each saw nine diagnoses of anaplasmosis. Sagadahoc and Waldo counties had none, according to data provided by the Maine Department of Public Health, which provides much information about vector (tick)- borne illnesses, and is a resource recommended by many doctors.
In 2013, Knox had 27 cases of anaplasmosis, Lincoln 10, Sagadahoc 3, and Waldo 3.
Tickborne Diseases of the U.S.
In the U.S., some ticks carry pathogens that can cause human disease, including:
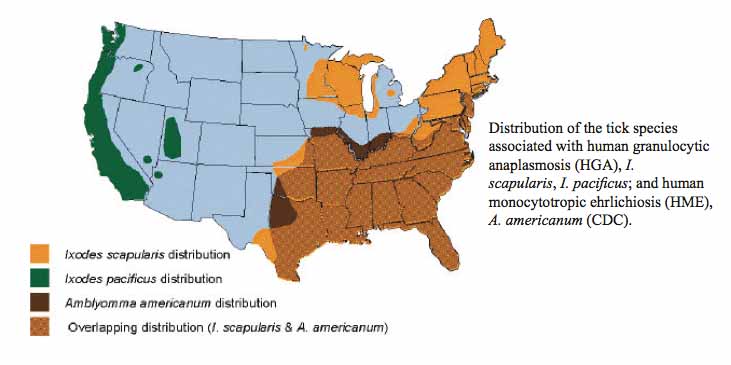
Anaplasmosis is transmitted to humans by tick bites primarily from the blacklegged tick (Ixodes scapularis) in the northeastern and upper midwestern U.S. and the western blacklegged tick (Ixodes pacificus) along the Pacific coast.
Babesiosis is caused by microscopic parasites that infect red blood cells. Most human cases of babesiosis in the U.S. are caused by Babesia microti. Babesia microti is transmitted by the blacklegged tick (Ixodes scapularis) and is found primarily in the northeast and upper midwest.
Borrelia miyamotoi infection has recently been described as a cause of illness in the U.S. It is transmitted by the blacklegged tick (Ixodes scapularis) and has a range similar to that of Lyme disease.
Colorado tick fever is caused by a virus transmitted by the Rocky Mountain wood tick (Dermacentor andersoni). It occurs in the the Rocky Mountain states at elevations of 4,000 to 10,500 feet.
Ehrlichiosis is transmitted to humans by the lone star tick (Ambylomma americanum), found primarily in the southcentral and eastern U.S.
Heartland virus infection has been identified in eight patients in Missouri and Tennessee as of March 2014. Studies suggest that Lone Star ticks may transmit the virus. It is unknown if the virus may be found in other areas of the U.S.
Lyme disease is transmitted by the blacklegged tick (Ixodes scapularis) in the northeastern U.S. and upper midwestern U.S. and the western blacklegged tick (Ixodes pacificus) along the Pacific coast.
Powassan disease is transmitted by the blacklegged tick (Ixodes scapularis) and the groundhog tick (Ixodes cookei). Cases have been reported primarily from northeastern states and the Great Lakes region.
Rickettsia parkeri rickettsiosis is transmitted to humans by the Gulf Coast tick (Amblyomma maculatum).
Rocky Mountain spotted fever (RMSF) is transmitted by the American dog tick (Dermacentor variabilis), Rocky Mountain wood tick (Dermacentor andersoni), and the brown dog tick (Rhipicephalus sangunineus) in the U.S. The brown dog tick and other tick species are associated with RMSF in Central and South America.
STARI (Southern tick-associated rash illness) is transmitted via bites from the lone star tick (Ambylomma americanum), found in the southeastern and eastern U.S.
Tickborne relapsing fever (TBRF) is transmitted to humans through the bite of infected soft ticks. TBRF has been reported in 15 states: Arizona, California, Colorado, Idaho, Kansas, Montana, Nevada, New Mexico, Ohio, Oklahoma, Oregon, Texas, Utah, Washington, and Wyoming and is associated with sleeping in rustic cabins and vacation homes.
Tularemia is transmitted to humans by the dog tick (Dermacentor variabilis), the wood tick (Dermacentor andersoni), and the lone star tick (Amblyomma americanum). Tularemia occurs throughout the U.S.
364D rickettsiosis (Rickettsia phillipi, proposed) is transmitted to humans by the Pacific Coast tick (Dermacentor occidentalis ticks). This is a new disease that has been found in California.
The main carriers of ticks in Maine are mice and deer, and they migrate via birds. Predators of ticks — those animals that consume ticks — are limited. Guinea fowl, chickens and turkeys eat them, and some birds, but there is little other wildlife that finds them palatable.
An outdoorsman, Hand is not one to fuss about insects. He pulled the tick off, estimating it had been there for 12 hours, and left on vacation with Amy and their two sons, Stephen and Zach, to New York City. They saw shows, museums and danced through April vacation, and then came back to Maine.
A few days later, he fell asleep on the couch watching television. He woke up at 10 p.m. with the chills, a temperature of 102.7, and headaches, “crazy headaches,” said Hand. “But they went away.”
That was Monday night. On Wednesday, he had an appointment to see the doctor. His fever had diminished, and the doctor said: ‘You’ve got a cold or something. You have to work through it. Take Tylenol for the fever.’
There was a brief conversation about the tick bite, and that was it.
Hand considered himself on the mend and went dancing with Amy. He also returned to work, albeit with a low-grade fever. And headaches.
Almost a week later, on Mother’s Day, May 8, he grabbed a rake and began tackling the yard.
“Around midmorning, I tried to broom gravel and said to myself, ‘I can’t do this.’ My whole body was dead.”
He rallied for Mother’s Day, taking his mother and Amy out to dinner to the Lobster Pound at Lincolnville Beach.
When they got home, he had a splitting headache and a tight cough. He passed out on the couch.
On Monday, he revisited the doctor, and was told, again, ‘You have a cold. You are unlucky to get two bugs in a row. Here’s an inhaler.’
“He then sent my on my way,” said Hand.
Rough waters
The next day, Tuesday, Hand was lying on his couch, burning with a temperature of 103.7.
“The sweat was pouring off of me and I had a hard time breathing,” he said. “I tried using the inhaler and took Tylenol. The next hour my temperature was at 102.9 but I still couldn’t breath.”
He got up but could not navigate the hall.
“I lay flat on my bed and could not talk,” he said. “That’s when Amy said, ‘we’re going to the hospital.’”
Emergency room doctors examined Hand, and he was wheeled to a hospital room, one with a view shed over Penobscot Bay (“I lay looking out over the ocean most of the time,” he said.)
“My temperature kept going up and down, and I was on fire, with water pouring off of me,” he said. His pulse rate was 113 and his blood pressure was low. Hospital crews ran fluid into him, and fed him Vicodin for the headache.
By Wednesday, “it was the worst,” he said. He wrote a short Facebook post, telling friends he was there and not in good shape. The post had approximately 10 sentences.
“It took me forever to write that,” he said. “Forty-five minutes to write a post that should have taken 10.”
His blood oxygen levels were declining, from 92 to the 80s, and nurses began giving him oxygen. Normal pulse oximeter readings range from 95 to 100 percent, under most circumstances. Values under 90 percent are considered low.
Doctors told him that his kidneys were not working well, nor was his liver.
“Good thing Amy wasn’t there,” he said, grinning.
Wednesday was also the day doctors told Hand, “We don’t know what you have.”
So, they began a regiment of two kinds of antibiotics while they waited to for blood analysis.
“That’s when Dr. Eggena came in and asked me a lot of questions,” said Hand.
Mark Eggena and his wife, Cheryl Liechty, are the only two infectious diseases doctors in the Midcoast, and are well-respected practitioners at at Penobscot Bay Medical Center. When they arrive, the big guns have come out and patients usually feel a little more reassured.
Hand told Eggena about his April 20 tick bite, but no swelling, no bulls-eye rash.
On Thursday, Eggena returned and according to Hand, said: “We think we know what it is. We are going to start treating for it tonight.”
The diagnosis was anaplasmosis, a tick-borne illness. On top of that, Hand had developed pneumonia.
He started on the antibiotic Doxycycline, plus “something nasty yellow paste stuff I had to squirt into my mouth.”
The latter turned out to be mepron, which was empirical therapy for Babesia, and given to Hand while the doctors awaiting the tests.
On Friday, his pulse started to drop a bit and his blood pressure climbed back up to 90 over 60. The drugs were working.
Vector-borne illnesses
“In Maine the three most common pathogens that deer ticks carry are Lyme, Anaplasma, and Babesia, the latter being the new kid on the block,” Eggena said.
(There is also the virus Powassan, “and currently the only well documented tick-borne transmitted arbovirus occurring in the U.S. and Canada,” according to the Maine CDC. Powassan encephalitis is a serious illness caused by the Powassan virus. This virus was first recognized in the small town of Powassan, Ontario, in 1958. Due to the ability of the virus to cause encephalitis, it was and still is considered a serious tick-borne illness.”
How the bacterial organisms of Lyme, Anaplasma and Babesia infiltrate human cells is still being researched.
There is, said Eggena, “a lot we don’t understand on the cellular and molecular level.”
Researchers do know, however, that the organism Anaplasma infiltrates white blood cells. At the same time, the body realizes something foreign is invading it, and the body responds by boosting its white blood cell count, its defense mechanism.
Anaplasma likes to live in those white blood cells. As the blood travels through the spleen and liver, the normal route to clean the blood, the cellular debris from the bacteria begins to build. The spleen and liver are designed to filter out the debris, but they get overwhelmed by the increase in cells.
“They become inflamed and you have the hallmark inflammation of liver and spleen — nausea and vomiting,” said Megan Kelly, Maine CDC epidemiologist.
There can also be coughing and wheezing, and chest tightness, as the bacteria travels around. In some cases, some people will have problems with kidney function.
The symptoms and progression of Hand’s experience with Anaplasmosis was almost textbook. Symptoms are expected to surface seven to 14 days after a bite, and Hand’s started 10 days to a T.
But not everyone gets as sick as he did. Many people have much milder symptoms, usually fatigue, headache, body ache, and fever, and then feel dramatically better after 48 hours of Doxycyline, said Eggena.
“The majority of people make a complete recovery within weeks although the fatigue can sometime linger longer,” he said. “Certainly some people can become critically ill, but this is not the norm.”
Unlike Lyme disease, however, propholactic antibiotics are not recommended for Anaplasmosis. The antibiotics at that point would be useless.
“There are no studies to suggest that prophylactic antibiotics are effective in Anaplasmosis and taking a single dose of Doxy (80 percent effective for preventing Lyme) could possibly just delay the onset of symptoms,” said Eggena.
But, at the onset of symptoms — headaches, joint pain, fever, nonspecific “feeling really bad,” said Eggena — then patients are encouraged to see a doctor, who will likely run a Polymerase chain reaction (PCR) test that amplifies the DNA of the organism in the blood.
The PCR takes 24 to 48 hours, but doctors generally don’t wait. If the clues come together, such as tick exposure and flu-like symptoms, then they treat empirically, most likely with the antibiotic Doxycycline. That antibiotic also attacks Lyme.
Major problem
The Maine CDC and doctors are not tossing tick-borne disease off lightly. They want the public to know that it is a major public health issue, and not limited to spring, summer and fall.
“We had cases diagnosed in February and March this past winter,” said Kelley, who works primarily in the Midcoast.
She stresses that personal protection is important, but there is more to consider.
“If you live in the Midcoast and you have flue like symptoms when it is not flu season and you know you have had exposure to ticks, go to your health care provider,” she said. “I’d like people to advocate for themselves. Providers need the patients to be aware, and advocate. Personal protection is not enough anymore. We’ve been advocating for that for years.”
Personal protection — repellents, wearing pants and boots, tucking pant legs into socks, body tick checks — is elemental when hiking or working in the woods, or backyard, but there are broader discussions under way now. They concern how to manage property, one’s own backyard, and how communities treat deer herds and use of pesticides.
“There is information available for community leaders, town managers, local health officers, people who can bring this to communities to discuss and make decisions about how they want to handle this,” said Kelley. “Maybe they do nothing, or maybe they think about what pesticides or wildlife management they might or might not want to recommend.”
Monhegan tried treating deer on that small island where Lyme became prevalent. It did not work, so the community completely eradicated its deer population. The presence of Lyme diminished, although not entirely.
A similar process has been under way on Islesboro this past year, with special deer hunt parameters in place to stop the infection rate of Lyme in the human population.
Other, more localized and less intense management methods include (see Tick Management Handbook An integrated guide for homeowners, pest control operators, and public health officials for the prevention of tick-associated disease):
Keep grass mowed.
Remove leaf litter, brush and weeds at the edge of the lawn.
Restrict the use of groundcover, such as pachysandra in areas frequented by family and roaming pets.
Remove brush and leaves around stonewalls and wood piles.
Discourage rodent activity. Cleanup and seal stonewalls and small openings around the home.
Move firewood piles and bird feeders away from the house.
Manage pet activity, keep dogs and cats out of the woods to reduce ticks brought back into the home.
Use plantings that do not attract deer or exclude deer through various types of fencing.
Move children’s swing sets and sand boxes away from the woodland edge and place them on a wood chip or mulch type foundation.
Trim tree branches and shrubs around the lawn edge to let in more sunlight.
Adopt hardscape and xeriscape (dryer or less water demanding) landscaping techniques with gravel pathways and mulches. Create a 3-foot or wider wood chip, mulch, or gravel border between lawn and woods or stonewalls.
Consider areas with decking, tile, gravel and border or container plantings in areas by the house or frequently traveled.
Widen woodland trails.
Consider a least-toxic pesticide application as a targeted barrier treatment.
A new perspective
When Hand saw a post from a Facebook friend in early April mentioning a tick bite and asking for insight on how to medically proceed, he scoffed. Now, after his ordeal, he more wary of ticks, and more aware of the body’s response to a bite.
Not all ticks, and that includes deer ticks, carry infectious bacteria or viruses. Some are harmless. But there is no predicting why or how that happens.
“Some ticks carry some weird things,” said Hand.
Hand’s Lincolnville property sits close to Lincolnville Central School and he knows there are pockets of tick habitat in the woods.
He is continuing on his course of antibiotics, and is now back to 80 percent of his normal body strength. He had been forbidden by doctors to work out at the YMCA, which he usually does three mornings a week, but now he is back at it and is on the slow road to full health.
He has, however, strong words of advice for those who exhibit symptoms and suspect they have had a tick encounter.
“They have got to be demanding when they go and talk to their doctors,” he said.
Meanwhile, Kelley, the Midcoast’s epidemiologist, hopes that Maine, and its citizens, will advocate not only for themselves if they become sick, but that they will also advocate for more tick-borne disease research.
“Unless we know the enemy we do not know the best ways to assess rick of exposure and give strong prevention methods,” she said.
Editorial Director Lynda Clancy can be reached at lyndaclancy@penbaypilot.com; 207-706-6657
Event Date
Address
United States















 opens at Harbor Theater on Friday April 18 at 7 pm.")